
Refraint not restraint!
Exersides is based on the concept of “Refraint”, which refers to a humane, multi-level patient security system. Exersides contains and deflects vital equipment so patients can have earliest mobilization. While it may seem counter-intuitive, agitated patients may actually do better with less restraint. In many cases, their agitation stems from the sensation of being restrained or confused from sedation.
Once the restraints are reduced or removed, agitation can actually be reduced, leading to a calmer patient. Of course, patients and staff must be safe. That’s what’s great about Exersides. With the exercise strap or no strap, safety is designed into the Refraint. It can quickly revert to a restraint when needed. The concept of Refraint is supported by several initiatives designed to improve critical care, including:
- ERAS: Enhanced Recovery after Surgery
- ICU Rehab
- ABCDEF Bundle
- PICS Initiatives
- ICU Liberation

What's so bad about traditional restraints?
Refraint and Agitation Reduction
Traditional restraints can create a downward spiral leading to delirium, ICU-acquired weakness and culminating in Post-ICU Syndrome. The SPIDAR Web below illustrates that Sedation, PICS, Immobility, Delirium, Agitation and Restraints are all intertwined like a web, each one connected with another.
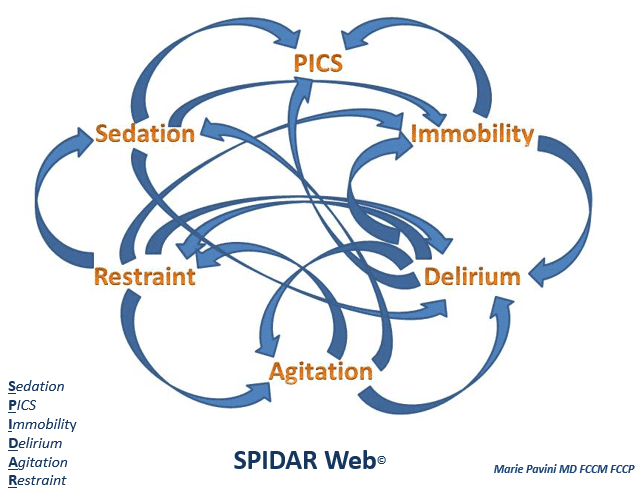
SPIDAR WEB
- Sedation leads to: Immobility, Delirium and PICS
- PICS (post-intensive care syndrome) results from: Sedation, Immobility, and Delirium
- Immobility leads to: Delirium, PICS and Agitation
- Delirium leads to: Immobility, PICS, Agitation (active), Immobility (passive), and Restraint
- Agitation leads to: Sedation, Delirium and Restraint
- Restraint leads to: Delirium, Sedation, Immobility, and Agitation

Refraint & Sedation Minimization
How do I minimize sedation and restraint?
First minimize sedation (chemical restraint) to a comfortable level for the patient that allows the most interaction or non-agitated movement. Then, select a level of restraint, or Refraint, to match the patient’s predictability for safe arm movement. Repeat this process until both sedation and restraint are completely minimized and the patient can safely move.
Do I need extra sedation for Exersides?
Definitely not. The purpose of Exersides is to promote non-agitated movement. You may find that if a patient is allowed to move, they may be less agitated and therefore require less sedation. Try it!
Do I need a sitter for Exersides if the patient is not sedated?
No. As long as the nurse chooses an appropriate Exersides configuration based on the predictability of the patient, safe arm mobility is possible.
We don’t use restraint – only versed and fentanyl.
Newsflash: Those are sedating and considered chemical restraint. That said, patients may need some amount of sedation to have non-agitated predictable safe arm movement. Challenge yourself and see how low you can safely go.
Do I need to stop all sedatives to use Exersides?
No. Some patients do not require any sedation ever and some do. If patients are allowed to move, they may require less. Always minimize.
What happens if the patient becomes agitated and moves too much?
Agitated movement is not good. It is better to find the least amount of sedation required by the patient than to select the next more restrictive level of Exersides. Minimize sedation first, then minimize restraint.
Refraint & PADIS 2018 Guidelines
The 2018 PADIS Guidelines call for more attention to restraints and caution that sedation is also a form of restraint. Numerous negative consequences associated with traditional restraints include:
- Higher benzodiazepine, opioid and antipsychotic medication use
- Increased risk for delirium or disorientation
- More unplanned extubations and frequent reintubations Greater unintentional device removal
- Longer ICU length of stay
This is why the American College of Critical Care Medicine Task Force recommends “the least invasive restraining option capable of optimizing patient safety, comfort and dignity.” Exersides makes it easy to use Refraint to implement the PADIS Guidelines and ACCM recommendations. With Exersides, you can easily minimize patient restraint and sedation to ensure patient and staff safety.
Refraint & Early Mobilization
How early is ‘Early’?
Some hospitals wait 2 days before mobilizing patients! Exersides allows mobilization the MOMENT the patient is able.
How often should I mobilize my patient?
Many patients only receive physical/occupational therapy sessions for 1/2 hour per day! Exersides allows movement 24 hours per day at the patient’s own pace.
Who is needed to mobilize a patient?
Most hospitals require a Physical Therapist, Occupational Therapist, Respiratory Therapist, and a Nurse or a Licensed Nurse Assistant to mobilize patients. Exersides allows patients to move themselves and perform their own Active Range of Motion!
Is Early In-Bed Mobilization safe?
Certainly, but nursing judgement is required to assess a patient’s readiness for safe movement. Fortunately, there are several levels of mobility to choose from and you will find one that is right for you and your patient.
Can Family be involved?
Most definitely! We believe it is healthy for family members to be involved in the healing process of their loved one. You may want to provide a general guideline for family to make the most of this precious asset.
